NSAIDs (Non-steroidal Anti-Inflammatory Drugs)
Used by 30 million Americans each day, NSAIDs are a unique category in their ability to reduce both pain and inflammation. With their non-addictive nature and well-established efficacy, NSAIDs have become a drug class of choice for many forms of pain and inflammation. However, they are widely known to cause gastrointestinal damage in normal use, a high-priority safety issue that has not been solved. Moreover, all NSAIDs both cause and then retard the healing of existing gastrointestinal ulcers. Notably, NSAIDs are also the leading cause of drug-related deaths in hospitals, primarily from gastrointestinal bleeding.
While acting as an anti-inflammatory in the body as a whole, NSAIDs (and other common drugs) can inflame and damage the gastrointestinal tract, leading to ulcers and bleeding in 20-25% of the population. This damage mainly arises because NSAIDs suppress prostaglandin production and block blood-clotting, impairing the body’s ability to maintain the mucosal layer that ordinarily protects the lining of the digestive organs.
Because NSAIDs are uniquely effective, several approaches have been attempted to protect the gastrointestinal tract while maintaining efficacy and not compromising safety:
COX-2 inhibitors
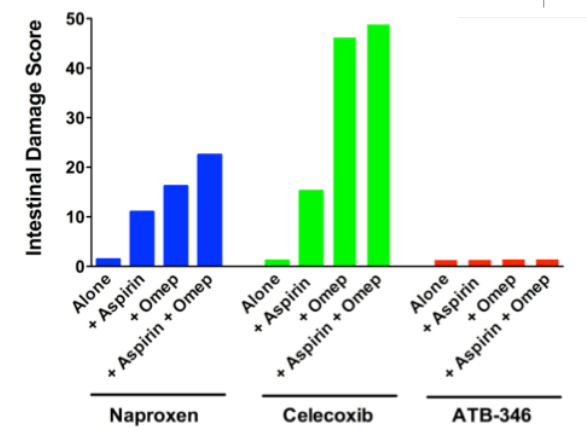
While traditional NSAIDs block both COX-1 and COX-2 enzymes, the 1990s saw the introduction of NSAIDs that specifically inhibited COX-2, based on the premise that NSAID-related stomach damage was primarily due to the effects of reduced COX-1. While these drugs were dramatically successful commercially, the FDA eventually removed several from the market, due to concerns that they increased the risk of cardiovascular events. Some COX-2 specific NSAIDs, principally celecoxib (branded as Celebrex), continue to be available under prescription but still pose risks to gastrointestinal health. Given today’s alternatives, COX-2 inhibitors remain the least damaging trade-off in effectiveness and safety for many physicians.
Additionally, the under-appreciated problems of using several drugs at once (“often known as “polypharmacy”, is an issue for COX-2 inhibitor users who also taking daily aspirin for secondary prevention of cardiovascular disease — even a relatively small amount of aspirin obviates the protective function served by the COX-2-specific mechanism.
Enteric coatings
Enterically-coated NSAIDs were introduced to prevent the digestion of the coated tablet in the stomach, thereby also protecting that organ from damage. However, enteric coatings are increasingly understood to be equally (or more) dangerous to patient health than uncoated NSAIDs. For example, while enteric coatings avoid stomach damage, they necessarily deliver intact pills (now absent the protective coating) into the more easily-damaged small intestine. As such, they cause more serious injury than they prevent. Secondly, enteric coatings are being shown to reduce the efficacy of the drug.